In the Okinawa and Amami regions, habu bites have been a serious problem that has affected people’s lives for a long time, and even in 1980, some 400 people were bitten and several died each year. Even in 1980, about 400 people were bitten and several died each year. With extermination and various improvements in the living environment, the number of bites was reduced to about 60 by 2020, and the use of antivenom has eliminated fatalities.
In 1895, antivenom serum produced by immunizing horses was used for treatment, and its effectiveness was confirmed. In Japan, the Research Institute for Infectious Diseases (later the Institute of Medical Science), headed by Shibasaburo Kitazato, used this method to immunize Amami Oshima habu venom to produce a prototype antivenom, which was completed in 1904.
In the early days, a mixed serum of habu and Mamushi was manufactured.
Currently, hub venom from Amami Oshima and Okinawa Island is being used.
In 1905, 118 people were treated with serum therapy in Okinawa and Amami, and although five people still died, the number of deaths was 1/3 of those without serum therapy, indicating that the therapy was quite effective. In the 1960s, it was often administered around the injured area.
However, the antivenom is not enough to cure the disease. In those days, it took a long time to reach medical institutions due to poor transportation, and antivenom was in liquid form, which could not be stored in rural areas without electricity. Since 1956, Yoshio Sawai and his colleagues at the Institute of Medical Science, the University of Tokyo, have conducted research on the purification, partial digestion, and freeze-drying of antiserum, and developed freeze-dried antitoxin (1959), which has improved both efficacy and shelf life. As a result, treatment with antitoxin became possible even in remote areas, and the fatality rate was reduced to 1%. Furthermore, unit price serum of habu and Mamushi began to be produced in 1961 and 1963, respectively.
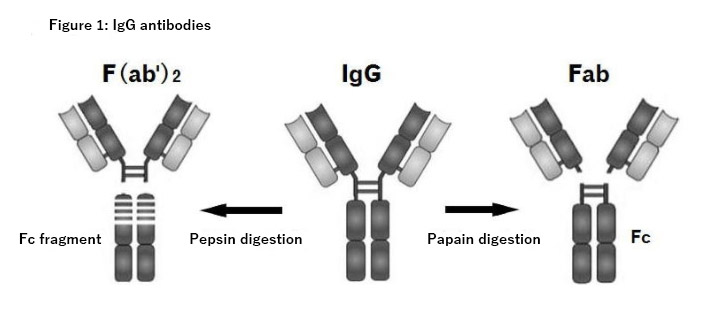
Since early antivenom contained inactive proteins unrelated to the antibody, these were separated and purified to produce antitoxins with only the gamma globulin fraction of the antibody portion. As impurities are removed, side reactions are reduced. In addition, pepsin digestion separates IgG, which has a molecular weight of about 150,000, into F(ab’)2, which has a molecular weight of about 110,000, and the Fc region, resulting in 80% of the antitoxin being F(ab’)2, 10% being IgG, and 10% being fragments of Fc. The smaller molecular weight of F(ab’)2, 10% of IgG, and 10% of Fc fragments in the antitoxin increases the speed of elimination from the body. In intramuscular injection, IgG is absorbed slowly and has a long half-life of 25 days, while F(ab’)2 has high tissue permeability and a short half-life of 9 days. Bovine antibodies are, of course, foreign to humans, and the longer they are in the body, the more antibodies are produced against the bovine antibodies, and the more likely they are to cause adverse reactions when administered again. Incidentally, in the U.S., the antitoxin CroFab (Crotalidae polyvalent immune fab) is currently being produced as a Fab with a molecular weight of 50,000 after papain digestion. (Fig. 1) The half-life is even shorter, about 15 to 23 hours.

Apart from antivenom, in order to reduce the severity of bite injuries, residents of some areas in Kagoshima have been vaccinated with Habutoxoid since 1970. However, its effectiveness has not been very clear. Currently, toxoid inoculation has been discontinued since 2002 due to the improvement of medical facilities and emergency transport system, which enables people to receive treatment in a short time.
In addition, local cleansing with EDTA solution (chelating agent), inotropes, adrenaline, and dextrose Ringer’s solution were administered. Since snake venom can be detected in the leachate at the site of injury, a small incision was sometimes made at the fang marks and continuous aspiration was performed with an aspirator if the patient came to the hospital in a short time. Since the protein in snake venom is a metalloprotein and its activity can be suppressed by chelating agents, the bite site is incised and washed with EDTA. Some doctors used tetracycline at the same time.
Tannic acid, used as a protein precipitant, was used for first aid cleansing because its astringent properties also neutralized habu venom. Based on the research that tannic acid extracted from astringent persimmons has higher neutralizing power than local tannic acid, a first aid kit of tannic acid solution was sold by the Tropical Medicine Association. Cepharanthine, which is still commonly used in the treatment of Mamushi bites, was also used in the treatment of habu bites at first, and there were research reports on its effectiveness, but after 1990, it was rarely seen and no longer used in treatment.
Broad-spectrum antibiotics are given to prevent infection, but some reports indicate that they are unnecessary because there have been no reports of infection from snakebites as well as from habu. In addition, tetanus toxoid is generally administered for animal bites, but there have been no reports of tetanus cases in hub bites. There have been few reports of tetanus cases due to animal bites, including overseas, with only a few reports of cases after venomous snake bites in Nigeria and Thailand.
Compartment syndrome is a problem in habu bites because the swelling is very severe. For this reason, a decompression incision is made, but because the fangs of the habu are as long as 1~2cm, the venom may be injected into the muscle, so a fasciotomy and cleaning is performed.
Reference data
Kobayashi Teruyuki “Viper” Bunshun Bunko 2000
Hifumi T, Sakai A, Kondo Y, et al: Venomous snake bites: clinical diagnosis and treatment. J Intensive Care 3:16, 2015, DOI 10.1186/s40560-015-0081-8
Blog Published on Oct 01, 2021 Changes in the treatment of venomous snake bites in Japan (from Dr. Atsushi Sakai)